

If you’ve been told you have a stubborn tendon or plantar fascia that just won’t quit, you’ve probably heard about shockwave therapy. Here’s a clean, evidence-based tour—minus the hype—of what ESWT is, how it helps tissue heal, which injuries respond best, and roughly how long recovery tends to take.
What is shockwave therapy?
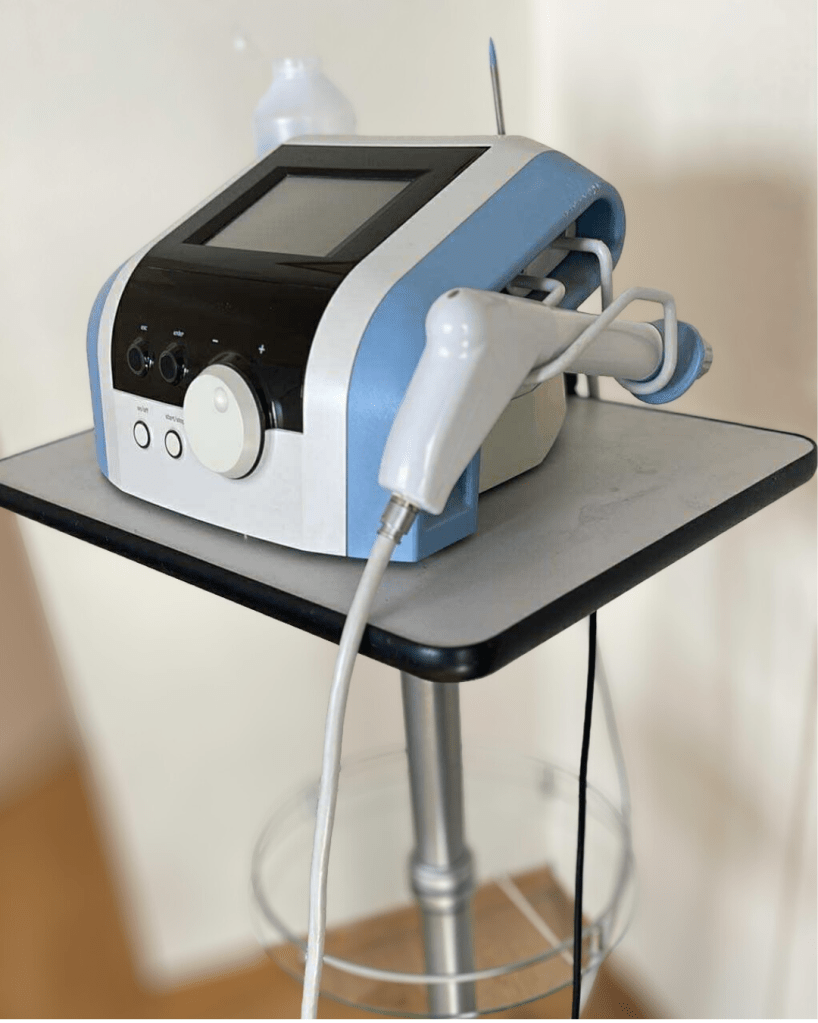
Extracorporeal shockwave therapy (ESWT) delivers short bursts of mechanical energy (pressure waves) into sore tissue from outside the body. There are two main flavors:
Focused ESWT (f-ESWT): concentrates energy deeper into a precise spot.
Radial ESWT (r-ESWT): spreads energy over a broader, more superficial area.
In musculoskeletal care, both types can help with chronic tendon and fascia problems. Typical clinical courses are 3–5 sessions about a week apart (the exact plan depends on the diagnosis and response). During treatment you’ll feel strong taps/pressure; it’s usually very tolerable and over in minutes. PMC
How does it help?
Research points to mechanotransduction (cells reacting to mechanical load), new blood vessel formation, collagen remodeling, and pain modulation (hyperstimulation analgesia). Think of it as a nudge that restarts a stalled healing process. PMCScienceDirectMDPI
Where Shockwave has the best evidence (and where it’s mixed)
Below is a practical snapshot for the conditions we treat most often in clinic. Evidence evolves; this reflects high-quality recent reviews and trials.
| Condition | What the evidence says | Typical plan & what to expect |
|---|---|---|
| Plantar fasciitis (plantar fasciopathy) | Strongest and most consistent benefits among common indications | 3–5 sessions. Many notice meaningful pain reductions by ~6–12 weeks, with ongoing gains toward 3–6 months. (PMC, PubMed) |
| Rotator cuff calcific tendinopathy | Best results with high-energy focused shockwave; improves pain/function and speeds calcific deposit resorption compared with low-energy regimens. | 3–4 sessions. Expect function/pain gains within ~8–12 weeks and better calcific resorption around 12 weeks; remodeling continues over months. (PubMed, BioMed Central) |
| Greater trochanteric pain syndrome (gluteal tendinopathy) | Trials show shockwave can reduce pain at 2–4 months; combining with targeted exercise is sensible. | 3–5 sessions + hip abductor loading. Expect improvement over 2–6 months. (PubMed) |
| Lateral epicondylitis (tennis elbow) | Shockwave is comparable—and often superior longer-term—to corticosteroid injection for pain and grip strength. Results vary by protocol. | 3–5 sessions + load management. Improvements by ~8–12 weeks, with continued gains by 6 months. (PubMed, arthroscopyjournal.org) |
| Achilles tendinopathy | Mid-portion: mixed but generally favorable when added to progressive loading; Insertional: RCT shows no added benefit over exercise. | 3–5 sessions (mid-portion) alongside a structured loading plan; expect 8–16 weeks for meaningful change, remodeling to 6 months. Insertional cases are exercise-first. (PMC, PubMed) |
| Patellar tendinopathy (jumper’s knee) | Evidence is mixed: recent studies shows little short-term benefit vs. placebo, though some trials show benefit vs. general conservative care or when combined with other therapies. Loading remains first-line. | Consider shockwave for persistent cases after ≥12 weeks of load rehab. If used, expect 8–12+ weeks before judging effect. (PMC) |
Recovery timelines above are averages from clinical trials/reviews. Individual pacing depends on chronicity, training load, the exact protocol (energy/dose), and how well rehab exercises are integrated alongside ESWT.
What happens at an appointment?
- Targeting & dosing: We locate the most tender/affected area(s) and select energy settings suited to the tissue depth (focused vs radial).
- Application: 1500–3000 pulses is common; it takes just a few minutes.
- Aftercare: You may feel sore for 24–48 hours. Prefer paracetamol/acetaminophen if needed; avoid NSAIDs right after treatment because mild inflammation may be part of how shockwave works. Gentle activity is fine; high-load or explosive work is re-introduced progressively. PMC
Safety, side-effects & who should avoid it
Common, short-lived side effects: transient redness, tingling, swelling, bruising, a “thuddy” ache.
Be cautious/avoid if: you are pregnant, active local infection, tumor at/near the site, significant bleeding disorders, treatment over lung/brain/growth plates, or certain implanted devices without specialist clearance. Your clinician will screen for these before we start. PMC
For device/indication-specific recommendations, we also follow the International Society for Medical Shockwave Treatment (ISMST) Guidelines (2024). shockwavetherapy.org
Curiously Aligned take: When do we recommend it?
- You’ve done the basics well (education, load management, progressive strength) for 8–12 weeks and still have significant pain or a plateau in progression.
- Your diagnosis is among the stronger-evidence group (plantar fasciitis, calcific shoulder, GTPS), or you have mid-portion Achilles that isn’t responding to a good loading program.
- You want a non-injection, non-surgical option that integrates neatly with rehab.
We’ll always pair shockwave with a targeted exercise plan and conservative therapy—that’s the engine; Shockwave is the spark!
Final thought
Shockwave isn’t magic—but it can be the missing piece when paired with smart rehab and load management, especially for plantar fascia pain, calcific shoulder problems, and lateral hip/gluteal tendinopathy. If you’re wondering whether ESWT fits your exact case, we can map a plan (with or without ESWT) that respects your sport, schedule, and goals.
Key references (peer-reviewed)
- Best-practice & mechanisms: Tenforde AS et al. PM&R. 2022. Practice recommendations; mechanisms & dosing (3–5 sessions; NSAID caution). PMC
- Plantar fasciitis: Lippi L et al. Systematic review/meta-analysis, 2024; JOSPT Heel Pain CPG, 2023. PMCPubMed
- Rotator cuff calcific tendinopathy: Brindisino F et al., 2024 (high- vs low-energy ESWT); Xue X et al., 2024 (systematic review). PubMedBioMed Central
- GTPS: Carlisi E et al., RCT 2019; Rhim HC et al., meta-analysis 2024. PubMed+1
- Lateral epicondylitis: Zhang L et al., meta-analysis 2024; Liu WC et al., meta-analysis 2022. PubMedarthroscopyjournal.org
- Achilles tendinopathy: Paantjens MA et al., systematic review 2022 (mid-portion vs insertional); Mansur NSB et al., RCT 2021 (insertional). PMCPubMed
- Upper-limb tendonitis overview: Xiong Y et al., meta-analysis 2024. Frontiers





Leave a comment